

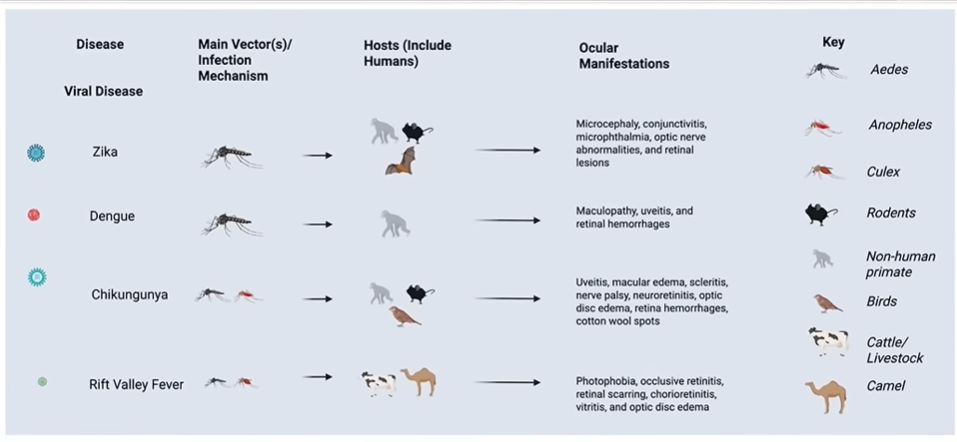
Chikungunya, Dengue Fever, Rift Valley Fever and Zika
The Coming El Niño: An Overlooked Catalyst for Vaccine Stocks?
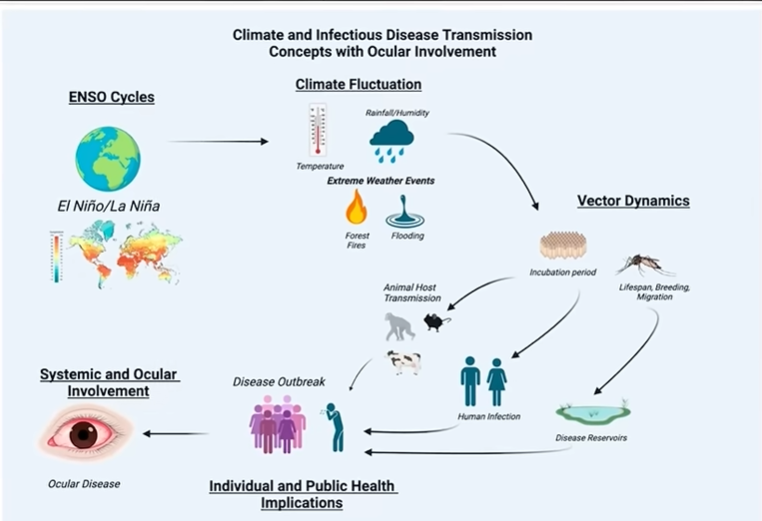
Investors obsess over interest rates, tariffs and AI. But Mother Nature may become one of the biggest market-moving stories over the next 12 months. Meteorologists are warning that an unusually strong El Niño could reshape weather patterns across the globe. History suggests that warmer temperatures and changing rainfall can expand mosquito habitats, increasing the risk of outbreaks of diseases such as dengue fever, chikungunya, Zika virus and Rift Valley fever in susceptible regions.
Public health officials don’t buy vaccines after epidemics—they prepare before them. If disease surveillance begins showing accelerating case counts, companies involved in vaccines, diagnostics, insect control and public-health preparedness could suddenly find themselves back on investors’ radar.
There are now multiple mainstream publications using the phrase “Super El Niño” in headlines. The important distinction is that many are using it as a journalistic label, while scientists and agencies like NOAA and the WMO usually stick with “strong” or “very strong” El Niño.
If these projections prove accurate, investors may soon be paying as much attention to Pacific Ocean temperatures as they do to interest rates. It pays (sometimes) to be early, as we were with the Corona Virus stocks in January of 2020.
Associated Press (2 weeks ago): “El Niño is here and scientists fear it’ll be big, bad and costly…” The AP reports that NOAA sees a 63% chance the event reaches historic intensity by fall or winter, potentially becoming one of the strongest on record.
National Geographic (4 days ago): “What a ‘super’ El Niño means for the planet.” The article discusses early forecasts suggesting this could be the strongest El Niño in a decade and explores the potential global impacts.
Yahoo News (20 hours ago): “El Niño has officially arrived…” It states that if a ‘super El Niño’ develops in 2026, it would be the first since 2015-16, citing NOAA’s historical comparisons.
The Guardian (April 13): “‘Super El Niño’ is officially here, scientists say.” The piece says forecasters believe the 2026-27 event could become one of the largest in modern history.
The Weather Channel: “What Super El Niño Means For Hurricane Season.” It discusses how an exceptionally strong event could amplify weather extremes and references recent research on “super El Niño” events.
World Resources Institute: “How Might a ‘Super El Niño’ Affect Food, Forests and Water?” This article explains how a super El Niño could intensify flooding, drought, and other climate impacts. (Links below)
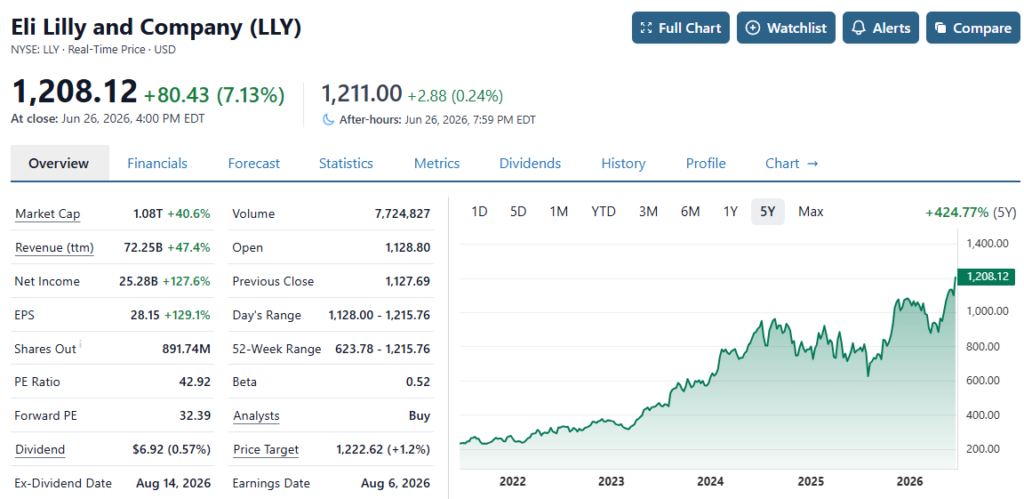
Industry transactions announced recently also suggest that the vaccine sector may be entering a new strategic cycle. A series of acquisitions announced by Eli Lilly (LLY) involving multiple vaccine-focused biotechnology companies highlights what may be an emerging shift in how large pharmaceutical organizations view infectious disease prevention, outbreak readiness, and vaccine infrastructure as long-term strategic priorities.
Eli Lilly’s recent acquisition spree may signal that large pharmaceutical companies are once again placing a premium on infectious disease prevention. In May alone, Lilly agreed to acquire three vaccine developers for up to $3.8 billion, targeting shingles, antibiotic-resistant bacterial infections and Epstein-Barr virus. The deals suggest that Big Pharma sees long-term value in vaccine platforms at a time when climate scientists warn that changing weather patterns could increase the risk of infectious disease outbreaks.
Lilly is buying companies focused on preventing infectious diseases before they become major public health problems. Management has described this as a strategy to prevent disease rather than simply treat it.
“One of the lessons learned from infectious disease emergencies is that preparation cannot begin after a crisis emerges Strengthening vaccine infrastructure, advancing next-generation platforms, and ensuring multiple sources of supply are investments that must occur before they are needed.” David Dodd, Chairman and Chief Executive Officer of GeoVax Labs Inc. (GOVX).
Final note: If Eli Lilly is buying vaccine companies before demand is obvious, who else might follow?
- Merck & Co.
- Pfizer
- Sanofi
- GSK
- CSL
Eli Lilly uses cash pile to fund untested drug development strategies, FT says
Superbug Watch List (January 27th) to Peak Gain
AVERAGE GAINS – 478%
Aethlon Medical, Inc. (NASDAQ: AEMD) $2.40 to $6.89 up 187%
Alpha Pro Tech, Ltd. (NYSE: APT) $6 to $41 up 650%
AstraZeneca plc (NYSE: AZN) $49 to $65 up 32%
BioCryst Pharmaceuticals, Inc.’s (NASDAQ: BCRX) $2.80 to $6.29 up 124%
Cerus Corporation (NASDAQ: CERS) $4.50 to $6.90 up 53%
Cleveland BioLabs, Inc. (NASDAQ: CBLI) $1.32 to $5.00 up 278%
Co-Diagnostics Inc (NASDAQ: CODX) $1.88 to $29 up 1,511%
Lakeland Industries, Inc. (NASDAQ: LAKE) $1.75 to $28 up 104%
Inovio Pharmaceuticals Inc (NASDAQ: INO) $4.24 to $33 up 701%
Moderna Inc (NASDAQ: MRNA) $21 to $95 up 352%
NanoViricides Inc (NYSE: NNVC) $8.50 to $19.20 up 123%
Novavax, Inc. (NASDAQ: NVAX) $7.80 to $151 up 1,835%
Vir Biotechnology Inc (NASDAQ: VIR) $19.95 to $75 up 275%
Average gain, up 478%, As they say, you can’t make this sh*t up! It’s insane.
List Two: Additions to Superbug WatchList
AVERAGE GAIN – 361%
Athersys (NASDAQ: ATHX) $1.85 to $4.38 up 136%
*Citius Pharma (NASDAQ: CTXR) $1.02 to $1.47 up 44%
Corbis (NASDAQ: CRBP) $5.55 to $8.78 up 58%
*Dyadic (NASDAQ: DYAI) $5.91 to $10.98 up 85%
iBio (AMEX: IBIO) $2.27 to $7.45 up 228%
Immuron (NASDAQ: IMRN) $2.57 to $28.99 up 1,028%
One Main (NASDAQ: ONEM) $28.50 to $44.80 up 57%
*Organicell (PINK: BPSR) $0.02 to $.29 up 1,350%
*Mitesco (OTC: MITI) $0.02 to $0.08 up 300%
Todos Medical (OTC: TOMDF) $0.03 to 0.13 up 333%
Average gain, up 361% – most compressed within 2-3 month period. This is actually the complete list with the biggest loser up 32% at it’s peak. What the.
Vaccine Stocks
- Moderna (mRNA pipeline)
- Bavarian Nordic
- NanoViricides, Inc.
- Emergent BioSolutions
- Valneva
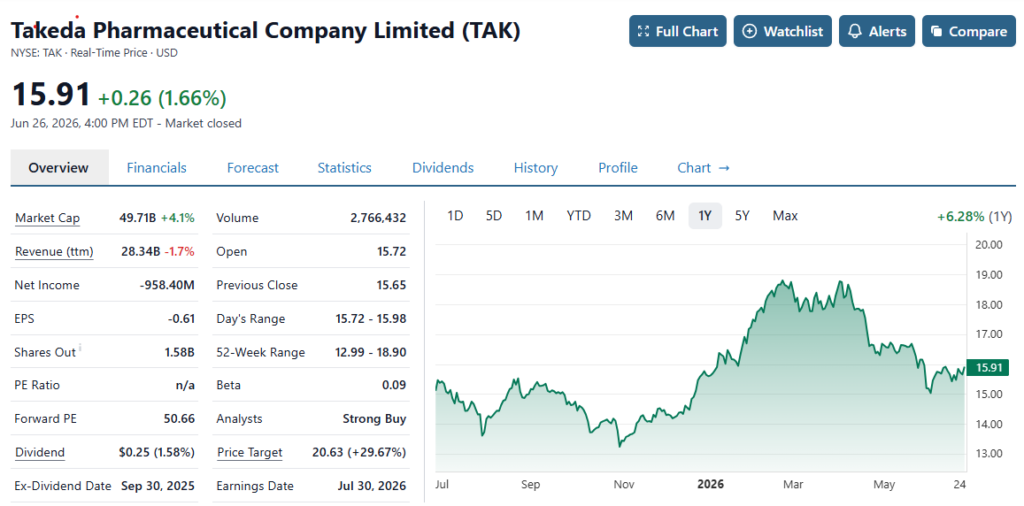
- Takeda Pharmaceutical (already markets a dengue vaccine)
- GeoVax (heading towards Phase III MPOX trials)
The Coming El Niño: An Overlooked Catalyst for Vaccine Stocks?
Climate scientists around the world are increasingly focused on the rapid warming of the equatorial Pacific Ocean, with many forecasting that the developing El Niño could strengthen into a moderate to strong event later this year. The latest outlooks from leading international forecasting centers indicate a high probability that El Niño conditions will persist through the end of the year, potentially reshaping weather patterns across much of the globe. Some experimental forecast models even suggest the possibility of a very strong event if ocean temperatures continue to accelerate. While no forecast is certain, confidence is growing that this could become one of the most closely watched climate developments in years.
For investors, El Niño is far more than a weather story. Powerful El Niño events have historically been linked to droughts, floods, heat waves, crop losses, and disruptions to global supply chains. They can also create environmental conditions that favor the spread of mosquito-borne diseases in certain regions, particularly where warmer temperatures and altered rainfall expand breeding habitats. Public health agencies closely monitor these patterns because diseases such as dengue fever, chikungunya, Zika virus, and Rift Valley fever have all demonstrated sensitivity to climate conditions in various parts of the world.
That raises an intriguing question for Wall Street:
Could a strengthening El Niño become an unexpected catalyst for companies developing vaccines, diagnostics, and infectious disease countermeasures? Governments rarely wait until an epidemic is out of control before responding. Instead, they increase surveillance, preparedness, and procurement as risks begin to rise. If forecasters are correct and El Niño intensifies over the coming months, investors may soon discover that one of the year’s most overlooked market themes isn’t artificial intelligence or interest rates—it’s the weather.
Moderna (mRNA pipeline)

Bavarian Nordic (BVRNY)

Adding Bavarian Nordic (BVNRY) $8.91, to Watch List.
NanoViricides, Inc. (NNVC)

Emergent BioSolutions Inc. (EBS)

Hantavirus cases spark brief surge in pharma and biotech stocks — here’s why trading is so volatile
Valneva SE (EPA:VLA)
LIVE QUOTE

Valneva SE Extraordinary Shareholders Meeting Transcript
Takeda Pharmaceutical Company Limited (TAK)
Takeda Canada Announces Positive Topline Results For Phase 3 LATITUDE Atlas Study For Psoriasis
Takeda’s AI-crafted psoriasis pill tops Bristol Myers’ Sotyktu in head-to-head trial
GeoVax Labs, Inc. (GOVX)

GeoVax Labs, Inc. (GOVX) Discusses Building a Resilient Infectious Disease Preparedness Strategy Focused on Ebola, Marburg, Hantavirus, and Mpox
TRANSCRIPT:
David Dodd
Chairman, President & CEO
Sure, John, and thank you for this opportunity. And I also want to not only welcome but thank all members of the Tribe Public as well as others who are participating in the day. Hopefully, you’ll learn a little bit, become interested in GeoVax and want to do a little bit of follow-up and I look forward to that.
Just to get started, let me just mention that my own background is 40-plus years within the pharmaceutical vaccine industry. It’s a wonderful industry in which to build a career, provides a tremendous amount of opportunity.
And what we’re talking about today is one of the reasons why I’ve always advocated that younger people starting their career consider this industry. And that is it presents continuous challenges.
I mean just think back to when we were all much younger 40-plus years ago when we started hearing about something called AIDS. It wasn’t even called that, some new disease. So there are always within our industry the opportunities for and the need for innovation for development on an individual basis, on an organizational basis.
And it’s quite an exciting industry. There are winners and losers, of course, but it’s a great industry in which to build one’s career. And so I’ve had the good fortune of starting very young and continuing to stay in this industry and work with it across many different opportunities. I would encourage anyone else to consider that.
So we are facing today a global challenge. But this global challenge is not new. It does seem that it’s happening more quickly and that is that emerging viral threats tend to test our limits of capability to be able to respond locally as well as globally.
And that continues to become perhaps an even greater challenge because as the world, in essence, gets smaller, we travel much more, we are seeing that emerging viral threats in fact, emerging pathogenic threats are happening, it seems like more frequently. They migrate much faster and we have to figure out ways to be able to respond to those.
But even more importantly, in response is really preparation and being prepared is what is most important for us. And so we’ve entered this persistent outbreak era. It was just a few weeks ago. Last month, we’re talking about Hantavirus and Ebola was, frankly, not on our mind, certainly not in the United States, but then certainly starting within earlier this month, we started hearing about these outbreaks in Democratic Republic of the Congo, in Uganda, of some new type of strain we’ve never heard about and what was going on there.
But let’s think about what we’ve been dealing with just within the recent past. We’ve been talking about what was originally monkeypox. We first started talking about that 4 years ago in 2022. Then it became known as Mpox, but more importantly, it went from an initial strain to a more virulent strain and now we have a new combination strain.
We’re seeing the first initial cases in the U.S. from that. Then we have the Bundibugyo or the BDBV Ebola outbreak. That’s the third version of the Ebola virus family that we’ve dealt with for, if you want to include Marburg. And we — as I mentioned earlier, we were talking just recently about Hantavirus. Now these are all things that provide tremendous amount of not only concern, but threats.
What’s happening starting probably next week? Well, what’s happening next week is we’re going to start seeing millions of people come to the United States for the World Cup. And when people are traveling as frequently as we do today globally throughout the world, what we’re doing is we may not think about it, but we’re carrying viruses with us.
Most of us have pretty good immune systems. So we don’t have to deal with that. But that threat increases tremendous exposure and threats on a global basis. How we deal with those and how we can be prepared to deal with those becomes critically important.
And it’s preparedness that is more important than simply respond. We respond when we’re in the middle, the eye of the hurricane, the middle of a threat, but we need to be preparing for it in between crises and that we have much to continue to learn.
Now MVA, John mentioned, we use a technology called modified vaccinia Ankara. MVA is the name of what was originally developed as the smallpox vaccine. It enabled us to eliminate smallpox from the world because previously, we used to use vaccinia.
Unfortunately, vaccinia, which is still around today, is contraindicated in certain populations, pregnant women, children and people with compromised immune system. We never would have eradicated the world of smallpox had we not developed a new version of it, which was good and it was safe for all populations and yet maintains a very robust immune response against smallpox in this case or what we could call pox viruses. So that became critically important.
It worked. It goes back to the last case of smallpox was announced in October of 1977. It was declared eradicated in 1980 because there had not been any more cases since that 1977 last case. And then we repurposed MVA beyond being simply a vaccine in terms of being a platform because it does not replicate in humans.
It’s exquisitely safe. It allows us the inclusion of multiple parts of a virus. So it’s known as a multi-antigen vaccine, which means you can take various components of pathogens. Even you can speculate about doing a single vaccine that would integrate Ebola Zaire, Ebola Sudan, Ebola BDBV, Ebola even Marburg.
All of these are very, very threatening, highly fatal. They have fatality rates up to 95%, the latest one has one approximately 40%, but being to put all those into the single vaccine and being able to deal with that. You can’t do that with mRNA. You can’t do that with other types of technologies such that AstraZeneca utilizes an adenovirus vector, different versions of that, can’t do it with the protein adjuvant types of technologies such as Novavax stuff. They can do combination, but they can’t integrate it into one.
You have the opportunity. It’s very challenging, but the opportunity to do it with MVA. So that type of platform enables you to take a single platform and address multiple outbreak opportunities and to do that in preparation, not simply in response.
So the core problem that drives everything is supply chain. People think it’s about just developing something that within the lab seems to work. That’s great. But if you can’t manufacture it, keep it stable, ship it, be able to utilize it, not in a highly frozen state, but in a real time, administer wherever it needs to be, villages in Africa, villages in the Asia-Pacific region, in the Southern Hemisphere where many of these emerging pathogens, we see the outbreaks.
If you can’t do it in those delivering millions and millions, hundreds of millions of doses if necessary, then all you have is a science project.
And far too often, we have something that’s exciting in the lab. It may even show that in a well-developed nation with all the access to supply chain elements such as the United States or in parts of Europe, frozen state delivery that it works. That’s great.
Now we go to the real world. What are these people doing today in Uganda, in the Democratic Republic of the Congo, the DRC. They are going from village to village, highly exposed, dealing with a highly contagious, in this case, the latest one being 40% plus in terms of fatal. But if you go to certain strains of the Ebola virus family, the filovirus family, you’re dealing with 95%.
In those cases, if you cannot give people and administer successfully, it doesn’t matter how well it might work in the United States, throughout the developed world, so to speak, it’s not going to help them and we’re going to have devastation. And that will not simply stay in that location, in that geography, it will travel because as people travel more and more coming to the World Cup, coming to other types of travel, they will be carrying that.
That’s what we’re seeing already with Mpox. And we’ve seen it previously with other parts of the Ebola family. We have to get away from that.
So I’m going to talk about a product that is close to initiating a Phase III trial. It’s called GEO-MVA. That is the MVA vaccine that is the version from GeoVax. It’s tied in with a global preparedness program.
The initial indication of the vaccine for which a Phase III, pivotal Phase III trial is scheduled to start in fourth quarter of this year is to target Mpox as well as smallpox. It’s very important because today, there is a limited insufficient supply of MVA vaccine in the world.
The European Medicines Agency, or EMA, the EU equivalent of the FDA has provided GeoVax an expedited pathway for development. They have waived having to do the traditional Phase I and Phase II clinical trials in humans. They’re only requiring a Phase III trial in healthy adults that will compare the immune response of our version of MVA with that of the only supplied product worldwide today, which is from a company out of Denmark known as Bavarian Nordic.
And they’re doing that because our MVA and that of Bavarian Nordic were initially derived from the same parenteral cell line. They are about as close as one could get and being, for all intents and purposes, identical.
And we’re targeted to start that trial in fourth quarter. And the reason why the EMA has done that is, first of all, because the extreme safety of MVA in general, but more importantly, the relationship between our MVA and that of Bavarian Nordic.
We have genetically sequenced our version of it and shown that it matches up 100% with all of what are known as the regions of interest or ROI that the regulatory authorities look at. So because of that, they’ve given us an expedited pathway.
We will initially be conducting a 500-patient trial. It will be healthy adults, 250 on our vaccine, 250 on the MVA-BN vaccine. We’ll be looking at 2 endpoints. One will be neutralizing antibody and the other will be the sero conversion rate.
And that will be started as we have targeted right now, fourth quarter of 2026. We’ve already manufactured all the product. It’s been packaged in the vials. It’s ready to go. We’ve selected our CRO, our clinical research organization.
We’ve selected where the sites are going to be and we have it set up so that when the trial starts, it will be completed with all 500 patients within 12 weeks. That’s essentially 3 months. We’ll have the readout of that in the middle of next year and that will be based upon those 2 endpoints that I talked about, neutralizing antibody and seroconversion rate.
Why are we so confident that we will show noninferiority? The criteria we’ve been given that are the basis for registration or marketing authorization is to demonstrate noninferiority on those 2 measures of our GEO-MVA to MVA-BN. And the reason why is we share the same lineage, we have the 100% match with genetic sequencing.
We utilize for all intents and purposes, the same manufacturing process, the same dose and the route of administration we’re following. We have the expedited pathway. We’ve been waived for Phase I, Phase II. And with that, we’ll be going forward.
We feel that with this, we will be able to demonstrate that. If that all works out, we will — and we’re able to demonstrate that we have noninferiority on those endpoints, we will then pursue emergency use licensing with the WHO and we’ll also pursue expedited approval with the EMA.
And then following that, we will then — assuming we are granted either EUL or the expedited pathway, we will then be conducting a 3,000 patient safety study that will be 3,000 patients, adults, not those — no efficacy measures required, just demonstrating that among the 3,000 patients that we will be doing, 2/3 of whom will be in Africa, 1/3 will be in the EU, that it’s a safe product, just further validating what we already know about MVA, that it does not replicate in humans and there are no adverse events otherwise, maybe a sore at the site of injection.
But other than that, we hope to show rather — which we’ve shown before in other studies rather benign any types of adverse events or tend to be localized related to the administration of the vaccine.
Now what does preparedness require? It requires manufacturing resilience because right now, if we look at it, there were approximately 7 million to 8 million doses of vaccine against Mpox delivered and utilized and administered in 2025.
However, there was an unmet need for further MVA vaccine in excess of 15 million doses, 10 million of which were specifically requested out of Africa, another 3 million thereabouts in the EU and then elsewhere, different contracting agencies, UNICEF and Gavi. We’ve got strategic stockpiles both across the world.
People are not aware of this, but in the U.S., Health Canada, U.K., Israel, Saudi Arabia, Middle East, throughout Asia-Pacific, most nations have stockpiles primarily developed related to the potential biodefense threat or bioterrorism threat of smallpox, but it’s the same vaccine. So it becomes utilized when we have Mpox outbreak.
So we’re looking for expanded capacity on a global basis, being able to do regional manufacturing and reliable access, not having to just build it when we absolutely need it, but build it on an ongoing basis. It’s not just a vaccine story. It’s an infrastructure story.
And this is what is most important. And the reason why is utilizing something such as the MVA-based platform, it allows us to move forward through cell line manufacturing, moving away from the historical somewhat very slow and cumbersome manufacturing process, same process we use, same process that Bavarian Nordic uses, but we’re migrating to a new process that will be scalable, reduced costs, reduced time to develop a batch will provide a tenfold increase over the current manufacturing process, being able to do twice the number of batches within the same time frame, we can only do one batch today.
So we have a multiplier effect and also doing it at lower cost and frankly, being able to transfer this technology so there could be localized manufacturing, which is not the case today. So we’re excited about it.
We hope to be able to transition to that new manufacturing technology within the next 3 to 5 years. But we will initially go to market with the same technology that is used to manufacture MVA today. Most important reason is it then provides a reference frame for being able to transition much faster to a new manufacturing process that would be cell line-driven and would have those attributes I just mentioned.
So why should anybody who’s thinking about potentially investing in GeoVax be interested in it? And first of all, I want to encourage you and employ you to do your own due diligence because there are always things that can trip people up.
So our current plan is and what we’re dealing with today is a very large and expanding market. I mentioned there were around 8 million doses last year. That translated last year into $700 million. That was the Bavarian Nordic product, the traditional vaccinia product with its limitations because of the contraindications. There’s also a product out of Japan that also carries those same limitations of contraindications.
So the Bavarian Nordic product did approximately $500 million in sales last year in U.S. dollars equivalents. There were around another $100 million, almost $150 million from the traditional vaccinia product and then about another $50 million for the product out of Japan, which is from KM Biologics.
In total, that gives you about $700 million in the total market. However, the demand that was requested that could not be met is an additional $1.3 billion. Our focus will be to go after what is being unmet, not to directly compete with someone who’s already supplying because what is out there is larger than the entire market that was satisfied last year.
So we will be going after that. We’ve already started discussions with potential contracting agency. We consider this a highly derisked program because we have the expedited pathway. We’ve been waived the Phase I, Phase II trials. We’re focused on the immune-bridging 500-patient study with a midyear 2027 readout and we believe there’s a high likelihood of success because of the attributes we’ve talked about.
And although we’ll go to market with the current manufacturing, we are focused on moving forward in as timely a manner as possible to this new manufacturing process. And again, I want to emphasize, we’re anticipating that will be 3 to 5 years. So we’ll go to market with what we have for current — for regulatory reasons, important reason being able to supply, but we will then transition as quickly as we’re able to.
Now I want to turn — I want to also comment because we’re in the vaccine business. People over the last several years, certainly, we’ve seen more of reluctance from investors and others who might be funding for vaccine.
That seemed to end just the other day with Lilly’s announcement of spending approximately $4 billion to acquire 3 infectious disease-related vaccine players. And that is opening up and we’re starting to hear about it. We’re starting to hear inquiries and receive inquiries about it, that it looks like that is turning the corner on the consideration of the vaccine industry, especially for companies who are in late-stage development towards registration, such we now find ourselves with our GEO-MVA that, that has been providing somewhat of some momentum and interest in there.
We anticipate that other large players, not just people already in the vaccine industry, but players that are looking to have sustainable growth opportunities will continue to look at this because vaccines are absolutely critical in addressing emerging threats, especially pathogenic threats, both from a viral infectious disease as well as a bacteria.
We’re focused on the infectious disease viral standpoint. But again, we consider that a very positive for our industry, for players such as GeoVax potentially. It all takes, obviously, people to look at it, become familiar with the technology. It tends to due diligence have not conducted overnight, but we do believe that this is a real boost for those of us in the development stage, especially the late development stage of vaccines.
Now what is the opportunity ahead? Well, what we look at for us is a number of groups are looking at. The Africa CDC is very active, vocal and in need of instituting continental-based vaccine capabilities, being able to work with MVA.
We’ve been in discussions with the Africa CDC for the last 3 years in this. UNICEF and Gavi has an active process underway, building stockpile for GEO for products of MVA vaccine, specifically the MVA stand-alone vaccines such as GEO-MVA.
In Europe, HERA is driving the way WHO through the emergency use licensing pathway. In the U.S., under BARDA, HHS, we have a Strategic National Stockpile. Other such national stockpiles, as I mentioned, we have them in Saudi Arabia, throughout the Middle East.
We see it in Israel. We see it throughout in the U.K. We see at Health Canada. We see it in Australia. We see it in Japan. So it’s all over the globe, we’re seeing that there are stockpiles looking for MVA vaccine and MVA-based vaccine. That is what we are focused on as a company.
Pipeline optionality with the recent announcements about the latest outbreak in Ebola, I just want to remind everyone that we have previously successfully developed vaccines against Ebola Zaire. We showed 100% protection in a single dose and that one against Ebola Zaire.
Ebola Zaire has up to a 90% fatality rate. We’ve done Ebola Sudan. We’ve done Marburg. Marburg, the Angola strain of Marburg has a 95% estimated fatality rate. So we’ve worked on that. So we’ve done those 3 before, presented those at international conferences.
We’ve carried them all the way through nonhuman primate testing. So we continue to have interactions with government funding agencies and others such as CEPI or BARDA for the government side. And we’ll continue to listen and look at those. We are not currently actively working on the new strain because we are so focused on our GEO-MVA to bring that to fruition and to initiate that Phase III trial in the fourth quarter.
So let me just close and say this is really all about not just 1 product or not just 2 products. It’s all about what we need to be prepared because preparedness should be done in between crises.
Once we’re in the middle of one, we’re scrambling to try and get something developed. That’s what’s going on right now. You’re seeing a lot of energy, a lot of activity of people trying to address this new strain. They’re trying to play catch-up and that’s what we intended to do worldwide, not just one nation, but everyone.
And the industry — for the industry to move forward, especially companies, we will consistently be dependent upon the necessary funding that either comes from government agencies or NGOs that have a stake in all of this.
And with that and our capabilities, our expertise, our experience, we can move forward and better address such threats from a preparedness standpoint so that when the outbreaks do occur, we’re all ready. We already have product manufactured. We already have product distributed. It’s ready for administration as necessary. That is what we all need to be seeking.
And with that, I’ll end my presentation, and I’m happy to take any questions that may arise. And I’ll just hold this up in case any of the questions necessitate going back to a previous slide.
El Niño Meteorlogic Video Discussing Outbreaks Spread by Weather
Be forewarned, long and technical. Outbreak discussion starts at 25 minute mark, comparing 1991 to 1992 El Niño which affected 86 million people with drought and mosquito producing rains and floods.
This Could Become the Most Powerful El Niño Ever Recorded
Forward-Looking Statements
This release contains forward-looking statements regarding GeoVax’s business plans. The words “believe,” “look forward to,” “may,” “estimate,” “continue,” “anticipate,” “intend,” “should,” “plan,” “could,” “target,” “potential,” “is likely,” “will,” “expect” and similar expressions, as they relate to us, are intended to identify forward-looking statements. We have based these forward-looking statements largely on our current expectations and projections about future events and financial trends that we believe may affect our financial condition, results of operations, business strategy and financial needs. Actual results may differ materially from those included in these statements due to a variety of factors, including whether: GeoVax is able to obtain acceptable results from ongoing or future clinical trials of its investigational products, GeoVax’s immuno-oncology products and preventative vaccines can provoke the desired responses, and those products or vaccines can be used effectively, GeoVax’s viral vector technology adequately amplifies immune responses to cancer antigens, GeoVax can develop and manufacture its immuno-oncology products and preventative vaccines with the desired characteristics in a timely manner, GeoVax’s immuno-oncology products and preventative vaccines will be safe for human use, GeoVax’s vaccines will effectively prevent targeted infections in humans, GeoVax’s immuno-oncology products and preventative vaccines will receive regulatory approvals necessary to be licensed and marketed, GeoVax raises required capital to complete development, there is development of competitive products that may be more effective or easier to use than GeoVax’s products, GeoVax will be able to enter into favorable manufacturing and distribution agreements, and other factors, over which GeoVax has no control.
Further information on our risk factors is contained in our periodic reports on Form 10-Q and Form 10-K that we have filed and will file with the SEC. Any forward-looking statement made by us herein speaks only as of the date on which it is made. Factors or events that could cause our actual results to differ may emerge from time to time, and it is not possible for us to predict all of them. We undertake no obligation to publicly update any forward-looking statement, whether as a result of new information, future developments or otherwise, except as may be required by law. GeoVax is a client of Institutional Analyst, the publisher of the Biotech Stock Review and has been retained with a combination of cash and equity for ongoing progress, news coverage and research reporting for five thousand dollars per month.
El Niño Links
 $0.27, Up 42%, to Watch List.")
. Palantir’s Open Secure AI.")


 $7.22. We’re Up And Out, With a 301% Gain.")

 $0.27, Up 42%, to Watch List.")
. Palantir’s Open Secure AI.")
 Jumps 100%.")
{kind=link}